
Identifying High-Potential HCPs: Using AI Behavioral Signals and Next-Best-Action Models to Drive NBRx
Driving New-to-Brand Prescription (NBRx) growth in today’s pharmaceutical landscape requires more than expanding reach. As access to Healthcare Professionals (HCPs) becomes increasingly constrained and digital engagement channels multiply, the real competitive advantage lies in identifying and prioritizing the right HCPs at the right moment. This article explores how modern commercial teams are moving beyond traditional decile-based targeting and historical prescribing data to adopt AI-driven behavioral insights and next-best-action (NBA) models. Instead of relying on static lists, these advanced approaches analyze real-time signals—such as content engagement, channel preferences, clinical context, access barriers, and prescribing momentum—to identify HCPs with the highest potential to generate incremental NBRx (iNBRx). The article outlines five categories of behavioral signals that predict prescribing momentum and explains how NBA models transform these signals into coordinated field and digital actions. By recommending the right intervention, in the right channel, at the right time, these systems help remove adoption barriers, improve engagement relevance, and accelerate therapy uptake. Industry evidence suggests that organizations deploying omnichannel orchestration and NBA frameworks see improvements in call efficiency, engagement conversion, and targeted NBRx growth. To capture this value, pharmaceutical commercial teams must shift toward always-on decision models supported by unified data, closed-loop measurement, and strong governance. Ultimately, the future of HCP engagement is behavior-driven prioritization rather than volume-based outreach. Companies that operationalize real-time insight activation will be best positioned to maximize field impact, improve physician experience, and drive sustainable prescription growth.
By the team at PharmaServ
2026-03-11T10:12:24+01:00
The Fastest Way To Grow NBRx Isn’t “More Reach”—It’s Better HCP Prioritization
Access to Healthcare Professionals (HCPs) is tighter than ever. Inboxes are saturated, field time is guarded, and competition for clinical attention is fierce. Yet, pharmaceutical brands are still on the hook for aggressive New-to-Brand Prescription (NBRx) growth.
This creates a fundamental tension: commercial teams desperately need to drive NBRx, but struggle to identify which HCPs are truly high-potential right now versus those who just have historically high volume.
In this article, we will break down how modern commercial teams solve this challenge. You will learn:
- What “high-potential HCPs” actually means in 2026 commercialization.
- Which AI behavioral signals matter for predicting prescribing momentum.
- How next-best-action (NBA) models turn scattered signals into revenue-driving decisions.
- How this orchestration directly drives measurable NBRx lift.
With growing channel fragmentation, faster therapy adoption cycles, and mounting pressure to prove the ROI of HCP engagement, relying on historical data alone is no longer a viable strategy.
The Current Problem: Why Most HCP Targeting And Engagement Still Misses The Real NBRx Upside
For decades, pharma has relied on a familiar playbook: decile-based targeting, static segmentation, broad specialty lists, and scoring based on the “last campaign.” These legacy models are broken. They rely on slow insight cycles, maintain rigid channel silos between field and digital, and suffer from inconsistent measurement.
This reliance on outdated data creates two massive blind spots:
- The “False Positives” Problem: High writers aren’t always high growth. Historical volume often masks market saturation, entrenched competitor loyalties, or a lack of new patient starts.
- The “False Negatives” Problem: Emerging fast adopters rarely show up on traditional target lists until it is too late. By the time claims data reflects their new habits, a competitor has already captured their loyalty.
Industry data confirms the fallout of these targeting failures: when outreach is driven by "who wrote last year" rather than "who needs help today," engagement becomes irrelevant noise.
- Digital Fatigue: Over 60% of HCPs report high digital fatigue (IQVIA/ZS).
- Declining Access: Rep access continues to drop as "static list" outreach fails to provide value.
- Context Gap: Most promotional touches are poorly timed or lack relevance (McKinsey/Accenture)—a direct consequence of firing off campaigns based on historical data rather than real-time clinical behavior.
The result: wasted field effort, lower NBRx efficiency, and slower adoption. It means missing the critical windows created by guideline changes, formulary updates, or competitor launches.
The Shift: From “Who To Call” Lists To Real-Time, Behavior-Driven HCP Prioritization
The pharmaceutical landscape is currently undergoing a significant commercial shift. We now have access to a vast array of data points including digital engagement, content consumption, and practice access behavior. AI tools have reached a point where they can interpret these various signals continuously, providing a level of insight that was previously impossible.
Traditional targeting models struggle in this new environment because they are fundamentally backward-looking. In contrast, modern real-time engagement strategies analyze behavioral signals to reveal an HCP’s intent. This allows teams to identify a propensity to start or switch therapies long before the changes actually appear in claims data.
As a result, forward-thinking brands are moving away from static lists. They are instead adopting omnichannel orchestration and next-best-action models that link directly to commercial outcomes. This transition ensures that outreach is both impeccably timed and contextually relevant. Ultimately, this precision leads to higher NBRx conversion while reducing the friction of unnecessary or poorly timed touches.
Define The Goal: What “High-Potential Hcps” Actually Means (And What It Doesn’t)
A "High-Potential HCP" is not necessarily your highest volume prescriber.
Definition: High-Potential HCPs are those with the highest expected incremental new-to-brand-prescription (iNBRx) impact over a defined horizon (e.g., 4–12 weeks), given their patient access, barriers, and responsiveness.
Potential is about incremental lift (iNBRx). A doctor writing 100 scripts a month who won't write an additional script is low-potential; a doctor writing 5 scripts who could write 20 is high-potential.
To identify them, combine three critical lenses:
Clinical fit: Do they have likely eligible patients?
Adoption readiness: Are they showing intent and openness to new clinical info?
Reachability: Do they have channel access and respond to outreach?
The ultimate measurement anchor is expected incremental NBRx (iNBRx)—not vanity metrics like opens or clicks.
AI Behavioral Signals: Signal Types That Predict Prescribing Momentum
"Behavioral signals" are observable actions that correlate with an HCP's interest, barriers, and readiness. These signals typically combine first-party engagement data with external practice-context signals to identify emerging prescribing momentum.
Here are the five core signal categories that predict NBRx momentum:
1) Engagement signals (what they consume and how they respond)
Includes email opens/clicks, time-on-content, repeat visits to efficacy pages, and call-to-action clicks (e.g., sample requests).
- Interpretation: These signals indicate whether an HCP is in an educational or logistical phase. Rather than overvaluing every click, teams should use weighted scores with time decay to prioritize the most recent, high-intent actions.
2) Access and channel-preference signals (how they want to be engaged)
Tracks rep meeting acceptances/declines, preferred formats, optimal contact windows, and channel opt-ins.
- Interpretation: Enables omnichannel personalization. If an HCP's rep access drops, the system dynamically shifts them to a digital-first approach to reduce wasted touches.
3) Clinical and practice-context signals (who’s likely to have eligible patients)
Looks at specialty, procedure mix, site of care, payer mix, and guideline-related content interest.
- Interpretation: Grounds behavioral interest in real patient opportunity, preventing teams from chasing curious but "low-fit" HCPs.
4) Barrier signals (what’s stopping adoption)
Includes repeated visits to reimbursement pages, downloading prior authorization (PA) resources, or abandonment of access content.
- Interpretation: High barrier signals often mean an HCP is clinically ready to prescribe but is facing logistical friction. Addressing these hurdles is often the fastest path to unlocking NBRx lift.
5) Momentum and change signals (who’s trending up before NBRx shows it)
Looks at signal velocity: increasing engagement over 2–3 weeks, shifts toward highly specific access content, or suddenly becoming highly responsive to a rep.
- Interpretation: Trajectory matters more than a static score. Models should prioritize upward movers.
Next-Best-Action (NBA) Models: Turning Signals Into The Right Action, In The Right Channel, At The Right Time
An NBA model is a decision engine that recommends the most effective next step for each HCP based on brand goals, constraints, and real-time signals. Unlike brittle static rules, AI learns patterns and updates dynamically, optimizing for incremental NBRx.
Step-by-step: How an NBA system works end-to-end
Ingest signals: Unify field, digital, and 3rd-party data into a single HCP profile.
Engineer features: Transform data into features like recency-weighted engagement and momentum scores.
Predict outcomes: Estimate the probability of response and the expected iNBRx lift.
Choose the action: Select the highest expected value action under specific constraints (capacity, compliance).
Orchestrate and learn: Deliver the action, measure the outcome, and feed data back for closed-loop learning.
These learnings should also inform marketing strategy, helping teams refine messaging and campaign design based on which actions actually drive engagement and prescribing momentum.
What “actions” can look like
- Field actions: A rep visit with a specific objective (e.g., "Discuss prior auth workflow") or speaker invite.
- Digital actions: A personalized content hub recommendation or localized payer resource.
- Hybrid actions: Triggering rep outreach only after an HCP downloads an access guide.
- Medical actions: Routing an MSL compliantly for deep, off-label, or complex clinical questions.
Guardrails that keep NBA realistic (and compliant)
AI governance is non-negotiable. NBA requires frequency capping (to prevent fatigue), territory rules (for field trust), explainable AI (showing reps why an action was recommended), and airtight privacy compliance and data lineage.
Connecting The Dots To NBRx: How Behavioral Signals And NBA Actually Drives New Prescriptions
The pathway from behavioral data to a new prescription is a direct, causal chain. AI signals first identify an HCP’s readiness, allowing a Next-Best-Action model to deliver a message that removes a specific barrier. This intervention encourages initial trial starts, which then manifest as measurable NBRx lift in claims data.
Consider these scenarios:
- Scenario A: High clinical fit + rising momentum + access barrier. NBA recommends: Digital reimbursement toolkit, followed by a rep visit on PA workflow.
- Result: Friction removed, NBRx unlocked.
- Scenario B: Moderate fit + KOL event attendance + high digital engagement. NBA recommends: Targeted efficacy content sequence, concluding with sample info.
- Result: Curiosity converted to clinical confidence.
- Scenario C: High writer + declining rep access. NBA recommends: Reducing field pressure and shifting to a low-friction digital journey.
- Result: Share protected, field efficiency maximized.
Proof And Validation: What The Industry Evidence Says
Industry evidence for omnichannel ROI is mounting. Firms like ZS, McKinsey, and Deloitte note that brands using NBA models routinely see double-digit NBRx uplift in targeted segments, improved call efficiency, and higher engagement conversions.
To validate this internally, the gold standard is test vs. control design and incrementality testing. At a minimum, measurement should track:
- Incremental NBRx/TRx (iNBRx/iTRx)
- Time-to-first-write
- Share shift within the target segment
- Rep call efficiency
- HCP experience signals (opt-outs/complaints)
What This Means For Commercial Teams: Practical Implications
This transformation impacts the entire commercial operating model:
- Brand Teams: Shift from rigid campaign calendars to always-on decisioning; map content to specific barrier stages.
- Sales Leadership: Focus rep time exclusively on HCPs with the highest expected iNBRx, eliminating low-yield calls.
- Analytics/Ops: Prioritize data unification, define outcome metrics early, and operationalize frequent model updates.
- Compliance/Legal: Embed governance upfront; document permitted data uses and audit trails before algorithms run.
Ignoring this shift risks continued high spend without precision and slower adoption compared to AI-enabled competitors.
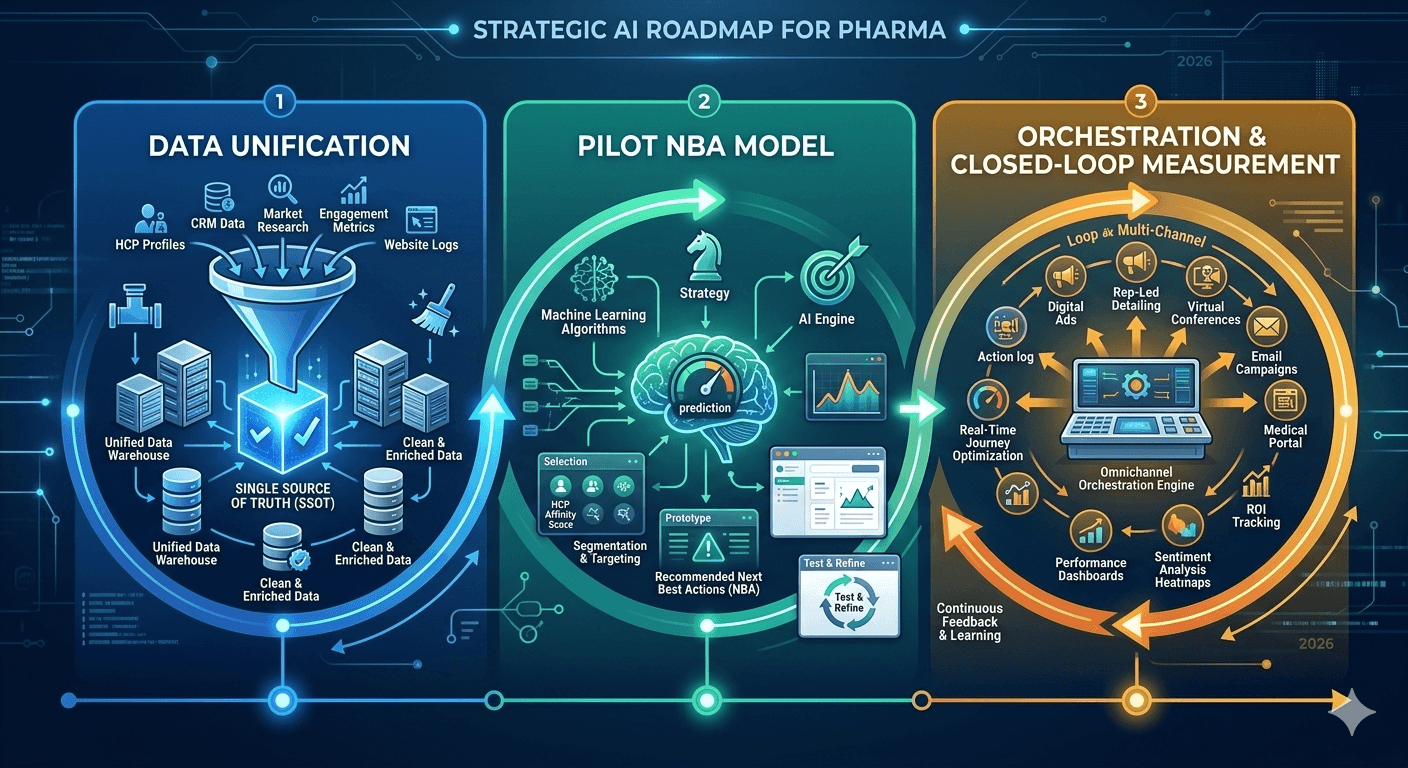
A Simple Implementation Blueprint: How To Start Without Boiling The Ocean
You don't need a massive IT overhaul to see value. Follow this phased roadmap:
- Phase 1 (0–6 weeks): Pick one brand objective (e.g., early adoption). Define your "high-potential" metric, unify a small set of high-signal data sources, and create a baseline score.
- Phase 2 (6–12 weeks): Deploy an NBA pilot in 1–2 regions. Establish strict holdouts and run closed-loop measurement.
- Phase 3 (12+ weeks): Scale across more channels, add complex barrier signals, automate learning cycles, and expand to additional indications.
Beware common failure modes: ingesting too many signals at once, lacking clear NBRx outcome definitions, and failing to secure field trust.
Next Steps: Let's Turn Signals Into Prescriptions
PharmaServ helps organizations implement behavioral analytics and next-best-action workflows that prioritize high-potential HCPs, remove adoption barriers, and improve NBRx efficiency.
Transitioning from static lists to real-time engagement doesn't have to be overwhelming. We can help you identify the signals you already have and build a pragmatic roadmap to activate them.
If you’re evaluating your HCP engagement strategy, PharmaServ can help you assess and activate real-time insight workflows.
Contact PharmaServ to explore how behavioral analytics and next-best-action models can improve your NBRx outcomes.
PharmaServ helps pharma and life science sales teams boost productivity with AI-powered workflows, real-time HCP insights, and compliant engagement.
Drive more calls, grow prescriptions, and make every connection count.
Contact
+12369785171
info@pharmaserv.co
4178 Dawson Street Burnaby British Columbia, Canada. V5C 0A1
Support
Policy
Copyright ©2026 PharmaServ